-
For Appointment
+91 98351 33046/+918318876486 -
Online Video Consultation Available
Consultancy Fee - ₹500/-

For Appointment
+91 98351 33046/+918318876486
Online Video Consultation Available

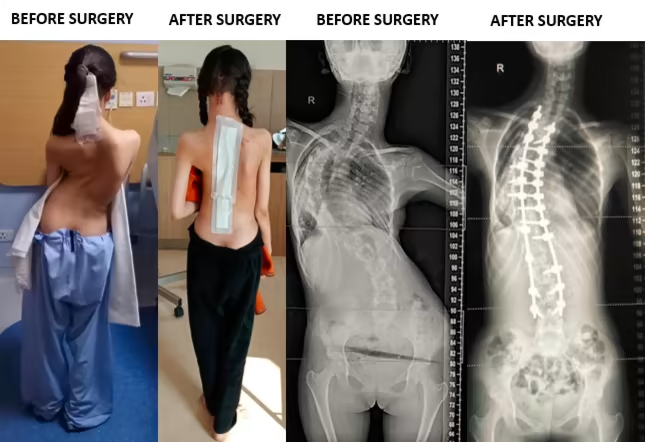
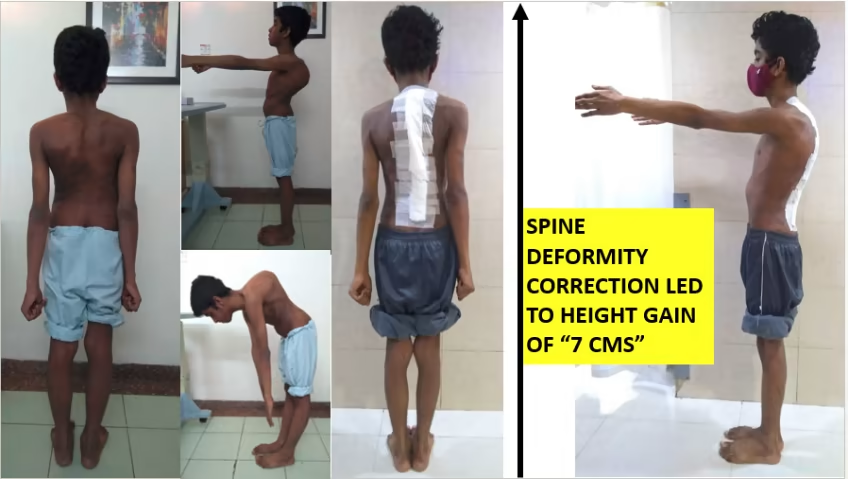
Everyone’s spine has natural curves. These curves round our shoulders and make our lower back curve slightly inward. But some people develop abnormal sideways curvature in the spine that is called scoliosis. The sideways bend results in the ribs becoming prominent on one side. This prominence is referred to as ribhump or razorback. This ribhump is perceived as a deformity by the patient and their parents and if it is severe it can result in a deformity that is obvious even when covered with clothes.
Patients with scoliosis may notice one shoulder to be higher than the other. They may have a shoulder blade prominent, asymmetrical breasts, asymmetrical waistlines and a tilted pelvis with one hip more prominent than the other. On an x-ray, the spine of a person with scoliosis looks more like an “S” or a “C” than a straight line. On Xrays, the severity of the scoliosis curve is measured by an angle called Cobb angle. For proper evaluation of scoliosis, your spine surgeon may order X-rays (AP and Lateral views) of Whole Spine (showing from neck to the hips in one film). Right and left bending Whole Spine X-rays and X-rays done under traction (pull) may be required if planning a surgery for Scoliosis. MRI of the Whole Spine will be required in all cases with Congenital Scoliosis and in Adolescent Idiopathic scoliosis where surgical correction is planned.
When Cobb angle is more than 50 degrees, scoliosis almost always needs surgery. Curves less than 30 degrees usually do not need surgery. Braces like Milwaukee brace and Boston brace may be used for curves between 20 and 50 degrees. Curves more than 80 degrees can compromise the functioning of heart and lungs and should always be corrected with surgery. Corrective surgery for scoliosis is usually performed from the middle of the back. The curvature in the spine is corrected using titanium screws and rods and the bones involved in the curvature are then fused together so that the curve does not progress any further with growth